Depression is common in the inpatient geriatric rehabilitation population, with studies reflecting close to one-third of the population experiencing depressive symptoms (Shahab et al., 2017). However, depression is frequently undiagnosed in this age group (Heidari et al., 2021) and is sometimes hidden by overlapping somatic symptoms. This can impact functional mobility and recovery (Ezema et al., 2019; Paolucci et al., 2019) and serves as a significant predictor of discharge functional independence measures (Shahab et al., 2017). Therefore, routine depression assessment can help identify patients at risk of decreased treatment gains if implemented early in the rehabilitation process. The purpose of this translational research study is to determine the significance of depression screening within the geriatric acute inpatient rehabilitation population and encourage routine depression screening within this population.
Literature Review
Within the physical medicine rehabilitation population, depression occurs in 18-33% of post-stroke victims (Medeiros et al., 2020), 30% of post-traumatic brain injuries (TBI) (Fakhoury et al., 2021), 29.3% of spinal cord injuries (SCI) (Peterson et al., 2020), 20% of acute coronary events (Helmark et al., 2022), and 9-47% of hip fractures (Heidari et al., 2021). Functional limitations, particularly independent activities of daily living (IADLs) and activities of daily living (ADLs), are associated with the onset of depression among the rehabilitation population (Ezema et al., 2019). In addition to negatively impacting functional status and patient outlook, depressive symptoms are associated with longer length of stay and falls while in hospital (Haines et al., 2015). Similarly, depression effects how patients heal and participate in the rehab process (Rao et al., 2020) and serves as a significant predictor of discharge functional independence measure or FIM score (Shahab et al., 2017). The key response is early identification of patients with distress, so health care providers can help provide reciprocal resources and support to patients (Vincent et al., 2015). Therefore, routine assessment of depressive symptoms is important to identify patients at risk for decreased treatment gains and should improve outcomes if implemented early within the team process.
Medical guidelines support screening for depression. Based on Class B evidence, the US Preventative Taskforce (USPTF) recommends screening for depression in the general adult population to ensure accurate diagnosis, effective treatment, and appropriate follow-up (USPTF, 2016). The Institute for Clinical Systems Improvement (ICSI) strongly recommends that clinicians routinely screen all adults for depression using a standardized tool (ICSI, 2016). Specifically, guidelines for stroke patients include assessing for emotional functioning and psychological needs (Dworzynski et al., 2015). Guidelines for TBI managements also suggests assessing for depression in relation to the current illness (Department of Veterans Affairs, 2016). Spinal cord injury guidelines suggest early assessment can lead to better treatment results (Colorado Division of Workers’ Compensation, 2021). Since risk factors for depression include medical illness with a biological cause such as stroke, medical illness perception, or health-related quality of life (American Psychological Association, 2019), the rehabilitation population carries a strong risk factor and should be addressed.
In addition to the rehabilitation population, depression is common in the elderly (Darwis & Safei, 2022), yet often goes undiagnosed within this age group (Heidari et al., 2021). Furthermore, the identification of depression among the elderly within acute rehab settings is complicated by overlapping symptoms of somatic diseases and disorders. One study by Shahab et al. found that 28-34% of older people admitted to an inpatient rehabilitation unit had clinically significant depression utilizing the GDS-15 and PHQ-9 tests, respectively (2017). Through depression screening within the older adult population on rehabilitation unit admission, this population can be better assessed in a timely manner. Rehabilitation teams can then help optimize patient outcomes and quality of life by recognizing early signs of depression (Vincent et al., 2015).
Methods
Per literature, depression has been connected to end functionality scores, adverse outcomes, and rehabilitation specific goals, so depression screening should occur in a timely manner. To assess the local depression prevalence and screening need, a depression screen utilizing the Geriatric Depression Scale (GDS) tool (Table 1) was implemented on admission to an inpatient rehabilitation facility (Sheikh et al., 1991). This review on the need for a type of standardized depression screen was based on the hypothesis that 1/3 of the patients were suspected to be at risk for depression. Findings are now being disseminated to encourage fellow clinicians to incorporate depression screening and translational research into clinical practice.
Setting
The depression screening was implemented on the admission assessment of patients sixty-five years or older admitted to a 41-bed inpatient rehabilitation center in the Southeastern United States. This center offered a wide range of debilitating disorders such as: CVA, TBI, SCI, amputations, generalized debility, cardiac or pulmonary related myopathies, polyarthritis, and other diagnosis meeting inpatient rehabilitation criteria. This unit utilized physicians, nurse practitioners, registered nurses, physical therapists, occupational therapists, therapy aides, speech therapists, and case managers daily to ensure appropriate and detailed patient-specific care in relation to patient illness or disease state. Daily assessment and open communication validated patient safety. The study exemption status was granted by both the hospital and university institutional review boards.
Sample
A convenience sample of 89 patients was instituted during the first trial from February 8, 2017 through February 28, 2017 and during the repeat trial from September 7, 2018, to November 7, 2018. Inclusion criteria for participants were age 65 or older, determined to be at least 75% reliable with yes/no responses per speech therapy evaluation and cognitive testing, able to provide informed consent, and the ability to participate in therapy efforts during hospitalization. Exclusion criteria were as follows: inability to respond reliably to yes/no questioning, inability to provide informed consent, or missed subjects due to short lengths of stay or inability to secure a private environment to administer the questionnaire.
The patients were admitted for deficits in either mobility, self-care, and/or cognition which are all considered functional deficits. Most patients had recently been discharged from an acute medical hospital setting with diagnoses of CVA, orthopedic fracture or amputation procedure, TBI, SCI, degenerative disorders, or general debility. Genders were close to equivalent in numbers. Insurance carriers primarily consisted of Medicare although the sample included all insurers as well as self-pay. Each patient worked with physical therapy and occupational therapy for one to two hours each per day; some also underwent speech therapy thirty minutes to one hour per day if it is deemed as beneficial to the patient-specific case. Each patient underwent a rehab stay reflective of debility and improvement potential which their length of stay varied from three days to over one month. Each subject was given a choice to participate in the proposed research and was provided with written consent as well as implications of data, possible harm, and their human rights.
Procedure
Geriatric Depression Screen Tool
The Geriatric Depression Scale (GDS) was selected for depression screening in this study due to its suitability for the older adult population, its simplicity, and its established reliability. The tool’s use of straightforward yes/no questions make it particularly advantageous for individuals who may have cognitive deficits, ensuring ease of administration and reducing the likelihood of misunderstandings. Furthermore, the GDS has been extensively validated and remains a trusted measure for detecting depression in older adults. According to Shahab et al. (2017), the GDS outperforms the Patient Health Questionnaire-9 (PHQ-9) in screening elderly individuals, with high sensitivity (86%) and specificity (79%). Additionally, the tool has been successfully utilized in the American Heart Association’s REHAB-HF trial, where it was trusted to screen for depression in older adults undergoing rehabilitation for acute heart failure.
While the PHQ-9 is commonly used, it includes items, such as low energy or difficulty concentrating, which can be influenced by other age-related health conditions like cognitive decline or medical illnesses (Shahab et al., 2017). In contrast, the GDS focuses more directly on emotional symptoms, minimizing the risk of misinterpreting somatic or cognitive issues as depressive symptoms. The Beck Depression Inventory (BDI) is another well-validated tool but is more complex and time-consuming for patients to complete. It also requires self-administration, which can be challenging for older adults with visual or cognitive deficits. Additionally, when administered by an observer, the BDI tends to result in lower reported depressive symptoms compared to self-reports (Stepankova Georgi et al., 2019). The BDI also includes questions about physical symptoms of depression, which can complicate interpretation in the elderly, where physical health issues may overlap with depressive symptoms. Lastly, the Cornell Scale for Depression in Dementia (CSDD) is more suited for individuals with cognitive impairment, making it less appropriate for a general elderly population where cognitive deficits are not a primary concern. Like the observer-rated BDI, the CSDD requires an external observer to complete the scale, limiting patient involvement and potentially hindering full disclosure of symptoms (Resnick et al., 2022). Given its targeted design, strong psychometric properties, and ease of use, the GDS-15 is often preferred for depression screening in older adults, making it well-suited for various clinical settings (Shahab et al., 2017) and the inclusion in this study.
Geriatric Depression Screen Implementation
Comprehensive clinician education of the GDS tool (Table 1) as well as its purpose and requisite within the rehab population was completed through PowerPoint presentation and open discussion. During February 8, 2017 to February 28, 2017, the GDS was implemented upon initial patient assessment within the first 24 hours of admission in aims of creating a standardized approach for depression screening within a timely manner. Data concerning patient scores were collected, then scores were averaged to identify and imply future patient needs in hopes of anticipatory treatment. As outlined in the GDS tool, a point was given for each answer in bold print. If the patient scored greater than 5 points, it was determined to indicate depression.
Retrograde Data Analysis
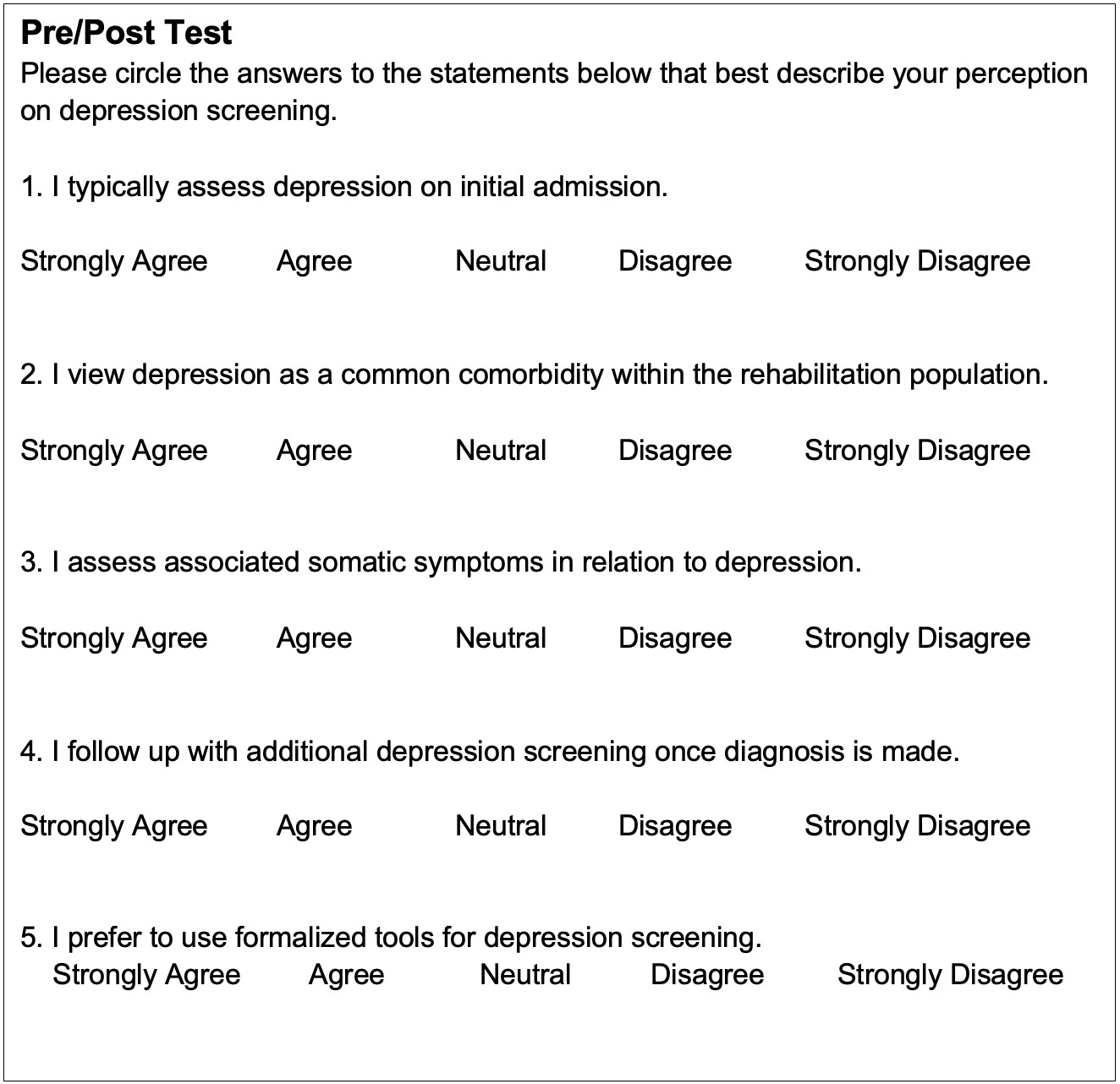
After completing the initial pilot study in February 2017, retrograde chart analysis was performed to examine the quantitative patient impact and a Likert-Scale Survey was performed to examine the qualitative clinician impact of standardizing depression screening on admission to the inpatient rehabilitation setting. For the quantitative review, a systematic chart review of admissions occurring three weeks prior, from January 18, 2017 to February 7, 2017, where a standardized depression screening tool was not utilized was compared to the following three weeks February 8, 2017 to February 28, 2017, where a depression screening tool was used upon new patient admission assessments to assess the timeliness and regularity of depression screens as well as the prevalence of depression. For the qualitative review, a Likert-Scale Survey was provided to clinicians pre-implementation and post-implementation to assess their perceptions on depression screening in order to determine the internal unit environment and chance of project change sustainability.
Repeat Geriatric Depression Screen Implementation
After determining impact of depression screening, a second pilot study was completed from September 7, 2018, to November 7, 2018. The GDS was implemented upon initial patient assessment, then scores were averaged to identify depression risk. As outlined in the GDS tool, a point was given for each answer in bold print. If the patient scored greater than 5 points, it was determined to indicate depression.
Data Analysis
The number of depression screens prior to GDS tool implementation on admission was compared to the February 2017 pilot study utilizing the GDS screen. Due to small sample size secondary to decreased patient census, the two sums were simply compared. Only four clinicians completed the Likert-scale survey following the February 2017 pilot study, so a general summary was concluded without SPSS data. Data from the February initial pilot study was significant to lead to a secondary pilot study in September-November 2018, though.
After the second pilot study was completed with a larger sample size, the total number of positive results from the two pilot trials in February 2017 and September-November 2018 were then compared using binomial analysis to determine the prevalence of depression in the unit and compare this to the hypothesized prevalence – one-third percentage. Finally, chi-square analysis was used to test the reliability of the 2-sample results.
Results
Geriatric Depression Screen Implementation
From February 7, 2017, to February 28, 2017, 25 patients aged ≥ 65 years were admitted to the local IRF. Twenty-four patients were screened; one patient in this age group was discharged before screening could be completed. Of these 24 screened, 8 were positive and 16 were negative. A total of 34.7% of participants were suggested by the GDS screen to require further evaluation for depression (Table 4).
Retrograde Data Analysis
After completing the initial pilot study in February 2017, a retrograde chart analysis was performed to examine the quantitative and qualitative impact of the depression screening. During the three weeks pre-implementation of the GDS tool from January 18, 2017 to February 7, 2017, only 6 of 20 patients were screened for depression during their admission. Post-implementation of the GDS tool, 24 of 25 patients were screen (Table 2); one patient was excluded due to severe cognitive deficit. Clinicians also completed a Likert-Scale survey (Table 3) which revealed increased positive scores (agree-strongly agree) regarding their perception on depression screening, significance, and intended follow-up. Both these quantitative and qualitative reviews demonstrated a positive impact of GDS tool implementation, so a second pilot study was completed to further analyze the need in local geriatric rehabilitation patients.

Repeat Geriatric Depression Screen Implementation
From September 7, 2018, to November 7, 2018, 78 patients aged 65 years and older were admitted to the IRF. 65 qualified to be screened; 13 patients in this age group were not screened due to unscheduled early discharge or inability to cognitively answer questions. Of the 65 patients screened, 22 tested positive and 43 tested negative. A total of 33.8% of the participants were recommended for further evaluation of depression (Table 4).
To compare the impact of the pilot studies, SPSS data processing was utilized. A binomial test indicated that the proportion of the total positive GDS screens was close to the hypothesized one-third of patients or 0.33, p = 0.265 (1-sided) (Table 5). A Chi-Square analysis was performed to verify that one sample year was not associated with more positive results. X2 (1) = 0.002, p = 0.964 (Table 4). This means that both years produced similar positive results, supporting the reliability of the two sample results from 2017 and 2018.
Discussion
Age, decreased physical function, and certain rehabilitation-specific diagnoses—such as cerebrovascular accidents (CVA), traumatic brain injury (TBI), spinal cord injury (SCI), and coronary events—are frequently associated with depression (Ezema et al., 2019). Unfortunately, depression is often overlooked in the geriatric population, where it may be underdiagnosed and undertreated (Heidari et al., 2021). Depression has been shown to significantly impact functionality (Paolucci et al., 2019) and contribute to adverse outcomes, including increased risk of falls, prolonged hospital stays, and challenges with reintegration into the community (Kapoor et al., 2019). Additionally, depression can interfere with rehabilitation goals and hinder recovery (Rao et al., 2020).
The relationship between depression and functional limitations is bidirectional, driven by a complex interplay of biological, behavioral, and psychosocial factors. Depression can worsen physical impairments by reducing motivation, energy, and engagement in physical activities. Conversely, functional limitations—such as loss of independence, chronic pain, and social isolation—can contribute to the development or exacerbation of depression. Over time, decreased motivation, cognitive decline, and reduced energy can result in lower participation in depression screening, making early identification and intervention even more critical. Given these challenges, it is important to implement depression screening in a timely manner. However, there is currently a lack of standardized depression screening tools specifically designed for rehabilitation patients. Therefore, the use of a consistent, evidence-based tool for depression screening in rehabilitation settings is strongly recommended.
The intent of this study was to evaluate the need for screening for depression in a local inpatient rehabilitation facility. This is solely translational research, in which a trusted tool was utilized, and its need was evaluated in clinical practice. The GDS screen was implemented based on the local patient population. This tool was chosen because it is a nationally accepted tool for this age group, but also for its short 15 question yes/no question format, which appeared to be easier for this particular IRF’s high rate of geriatric stroke patients. This IRF also provides services for TBIs, SCIs, orthopedic surgeries, trauma, critical illness myopathy, congestive heart failure, chronic obstructive pulmonary disease, and generalized debility. However, specific diagnoses were not documented, as this study was only intended to evaluate if the facility’s overarching needs a standardized depression screening tool.
The GDS’s 15 questions were then either printed for the patient to read and circle yes/no, or read out loud for the patient to answer per patient preference. During the process, none of the patients refused to be screened, and several expressed gratitude for the acknowledgment of their mental health. This process also allowed patients to elaborate on their deficits, fears, and questions regarding their diagnosis. Additionally, healthcare providers have acknowledged a better understanding of the extent of depression within the rehabilitation population during this process.
The pilot study revealed that approximately one-third of our IRF population aged 65 and older was at risk for depression. Given this significant proportion of patients showing depressive risk, we recommended the implementation of a standardized depression screening tool for the unit, with plans for its official integration in the next electronic medical records update. Following this, further research will be conducted to assess the frequency of depression and evaluate the outcomes of depression treatment. While the sample size was relatively small (89 participants) and the data were drawn from a single regional IRF, the findings demonstrate notable generalizability to the broader rehabilitation population, including both inpatient and skilled nursing facility settings. The results align with larger studies on depression in geriatric and rehabilitation populations, reinforcing the relevance of these findings across diverse rehabilitation contexts.
The dissemination of these results underscores the high prevalence of depression in the IRF setting. Since depression screening plays a critical role in identifying at-risk patients, influencing treatment and monitoring, we encourage rehabilitation healthcare professionals to prioritize depression screening. However, future evaluations should consider several limitations, including the need to assess multiple depression screening tools, develop specific pharmacotherapy and psychotherapy treatment plans, explore the impact of specialized rehabilitation units or specific rehabilitation diagnoses, and address potential challenges related to time and resource availability for effective screening and treatment.
Conclusion
Depression assessment needs to be implemented early within the rehabilitation team process, yet it is often overlooked, which underscores the effects of mental and emotional status on the healing process. Although depression is common in the elderly (Darwis & Safei, 2022), it often goes undiagnosed within this population (Heidari et al., 2021) and is complicated by overlapping symptoms of somatic diseases and disorders within the rehabilitation population. Since depression has been shown to affect functionality, adverse outcomes, increase falls and length of hospital stay (Paolucci et al., 2019) and affect rehabilitation-specific goals (Kapoor et al., 2019), depression screening should occur in a timely manner and the approach should be standardized on admission to the medical rehabilitation facility.
One out of three patients within an acute rehabilitation program were diagnosed and discharged on depression treatment, which demonstrates the magnitude of depression. Ultimately, mental health should be addressed as a comorbidity of both acute and chronic disabilities. Although depression may not be palpable or audible, it can be assessed. The fear of asking is infinitesimal to the fear felt by the patients. Depression screening can expose patients to silent suffering.
Funding Statement
The study was not supported by any funding.
Conflict of Interest declaration
The author declares that they have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.